
A spinal fusion removes the flexible elements of the spine, creating a solid block of bone throughout the fused area of the curve. This, in most cases, is performed with the addition of an instrumentation system of rods, hooks, wires, and/or screws. The instrumentation system is used to correct the curvature of the spine as much as possible, as well as to maintain stability of the spine in the postoperative period while solidification of the fusion occurs. The surgical approach to the spine can be either through an incision on the back (posterior) or an incision on the side (anterior).
The choice between a posterior (back) or anterior (side) surgical approach to the spine is a critical decision that depends on various factors such as the location of the spinal deformity, the surgeon’s preference, and the specific needs of the patient. Both approaches have their advantages and considerations in terms of access, visibility, and impact on the surrounding spinal structures.
Following spinal fusion surgery, patients often undergo physical therapy to help restore strength, flexibility, and mobility in the spine. Physical therapy plays a crucial role in the rehabilitation process, aiding in the recovery of normal function and reducing the risk of complications post-surgery. It is essential for patients to adhere to their physical therapy regimen to achieve optimal outcomes and long-term spinal health.
Primary care physicians also play a significant role in the management of patients undergoing spinal surgery. They are responsible for coordinating care, monitoring postoperative progress, and addressing any concerns or complications that may arise. Effective communication between the primary care provider, surgeon, and other healthcare professionals is essential for ensuring a smooth recovery and overall success of the surgical procedure.
Spine fusion surgery not only impacts the spinal column but also has implications for the spinal cord and surrounding nerve structures. The surgery aims to stabilize the spine, alleviate pain, and improve spinal function in cases of spinal deformity, degenerative conditions, or trauma. Careful consideration of the spinal cord and nerve roots is crucial during the surgical procedure to minimize the risk of potential damage and ensure favorable outcomes for the patient.
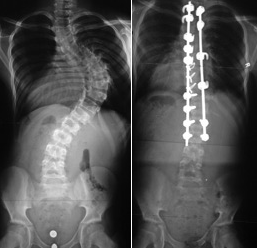
Figure 8b
Posterior Fusion
When doing a posterior spinal fusion the spinous processes, lamina and transverse processes of the spine are exposed. It is to these elements of the vertebra that the hooks, wires, or screws are placed to provide fixation of the rod to the spine (Figure 8a, b). Bone graft is applied to the exposed bony surfaces of the spine, which allow these vertebrae to subsequently grow together or fuse with bone connecting each of the vertebra to one another.
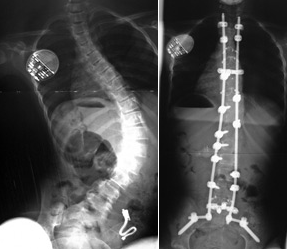
Figure 8a
Anterior Fusion
In some curve patterns, a similar correction and fusion can be performed via an anterior approach. This involves an incision on the side of the chest or abdomen to expose the front or anterior part of the spine. It is in this area where the vertebral bodies and discs are located. Fusion in this area involves removal of the soft disc material between the vertebrae and replacement of this tissue with bone graft, which will allow bony union or fusion between the adjacent vertebral bodies. Instrumentation systems that are applied anteriorly generally involve fixation to the vertebral body with a screw and connection between the screws with a rod system. This anterior approach can be done in the thoracic, thoracolumbar or lumbar regions, depending on the curve pattern.
Anterior and Posterior Approach
There are times when both an anterior and posterior approach to the spine is required. In circumstances when the curve is extremely rigid or the patient quite young (less than 10-12 years), approaches to both the front and back of the spine may be required. Much of the growth potential in the spine is located in the vertebral body adjacent to the disc. This growth center is responsible for vertebral body growth and causes much of the progression of the curvature that occurs during spinal growth. Therefore, anterior fusion is useful at decreasing or stopping the anterior vertebral body growth. Therefore, in young patients, anterior fusion is recommended. The anterior fusion may be required in combination with a posterior fusion and instrumentation if the curve cannot be instrumented anteriorly. When a curve is particularly large and rigid, correction may be inadequate if posterior instrumentation is done without removal of the anterior discs. Removal of the anterior discs in such a case increases the flexibility of the spine and allows for better correction of the deformity by the instrumentation system.
Minimally Invasive Techniques
Minimally invasive methods are also available for approach to the anterior aspects of the spine. In the chest this is done with what is known as a thoracoscopic approach. The endoscopic approach utilizes small incisions and video technology to view the spine. Specialized instruments are used to perform disc removal, instrumentation and fusion. In some cases, a posterior fusion is also required to perform the instrumentation portion of the procedure, although some curves can now be corrected with the endoscopic approach alone.
Learn about Surgical Risks and the Recovery Period.